

It was just past 3 a.m. when Reena Devi, 27, started bleeding. Her mother-in-law panicked. The nearest Primary Health Centre (PHC) in Banka, Bihar, was closed. There was no ambulance, so they pushed her into a tempo — a three-wheeled auto — and started toward the district hospital 34 km away.
Midway, near Katoria Chowk, Reena stopped breathing.
Her husband Manoj doesn’t speak much now. “She was alive when we started. But there was no one on the phone. No doctor. No vehicle. The hospital said later, Why didn’t you call 102? But how do you call when no one picks up?”
This is not one case. This is the daily truth of rural India, where women die not from disease but from distance, delay, and denial.
The Broken Chain of Care
In Latehar district of Jharkhand, the local Community Health Centre (CHC) has no gynaecologist. The labor room is under lock after 5 PM. ASHA worker Rina Kumari explains, “We try to get women to the hospital, but most deliveries happen at home. Ambulances don’t come to hilly villages after dark.”
When 19-year-old Sunita from Barwadih block started labor at night, she was carried for 4 km on a makeshift stretcher. The ambulance was called three times, never came. By the time they reached the CHC, the child was stillborn, and the mother was unconscious.
No complaint was filed. No one was held accountable.
Schemes on Paper, Silence in Practice
The Janani Suraksha Yojana (JSY) promises ₹1,400 to women who give birth in institutions. Yet, according to the 2023 NHM report, more than 46% of rural deliveries in Bihar still happen at home.
The Janani Express ambulance system — launched to provide 24×7 emergency response — has just 1 ambulance for every 45,000+ people in parts of Jamui and Garhwa. Many are non-operational due to unpaid diesel bills or driver shortages.
Data from RTI filed by local NGO Gramin Swasthya Sangharsh Samiti in 2024 shows:
-
34% PHCs in Bihar and Jharkhand lack functioning delivery rooms
-
48% of sanctioned doctor posts remain vacant
-
Only 12% of CHCs have a female doctor available full-time
Where Death is a Common Birth Companion
In Saharsa, Bihar, villagers have a saying — “Delivery ke samay dua bhi chhoti pad jati hai.” (At the time of childbirth, even prayer falls short.)
One ASHA worker shared off-record: “We are told to convince women to go to hospitals. But when we do, the hospital says beds aren’t available or staff are missing. What do we do? Sit beside her and pray?”
In the same district, three maternal deaths were reported in one week in April 2024. None made it to the hospital in time. Two were declared dead on arrival. The third died while searching for oxygen.
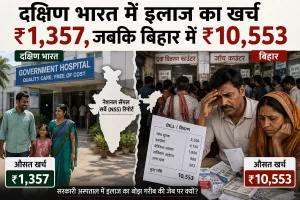
Where Poverty Screams Louder Than Pain
The Cost of Giving Birth
In Garhwa, Jharkhand, a woman named Savita Devi, aged 22, delivered her baby outside the hospital gate. The labor pains started at night. The ambulance was “unavailable”. When they reached the CHC by borrowed bike, the guard refused entry without ₹500.
Her husband Rajan, a migrant worker who had returned from Surat just a week earlier, said:
“They said the doctor was asleep. We were told to wait. But blood kept coming… I banged the gate, screamed. Nobody came.”
She gave birth in the open, on the mud-covered hospital steps.
The baby died.
She survived — barely.
Later, they received ₹1,400 under JSY but spent ₹7,000 on medicine, injections, and “entry fees”. Rajan sold his mobile phone and watch.

“Is My Life Worth a Phone Call?” — ASHA’s Silent Fight
In Jamui, ASHA worker Meena Kumari handles 34 villages. She earns ₹2,000–3,000 per month, often paid after 4–5 months of delay.
“We are the first responders. We carry women on our backs. But we have no ambulance, no gloves, no delivery kits. If the woman dies — it’s our fault. If she lives, the hospital gets the credit.”
When asked about training, she laughs. “Training is WhatsApp voice notes from supervisors. We Google symptoms now.”
In a 2023 ASHA union survey:
-
78% of ASHA workers in Bihar work more than 10 hours/day
-
Less than 5% have received emergency birth training in the past 3 years
-
82% reported harassment by hospital staff or families
The Silent Epidemic: Maternal Mortality
According to NFHS-5 and Ministry of Health data (2023):
-
Bihar’s Maternal Mortality Ratio (MMR): ~149 deaths per 100,000 live births
-
Jharkhand’s MMR: ~163 per 100,000
-
Both are significantly higher than the national average (~97)
But these are undercounted deaths. Many rural women die unregistered, at home, in fields, and in vehicles. Their names vanish in red tape. Their pain becomes folklore.
One local activist in Saharsa told us, “Maternal death is not even considered ‘news’ anymore unless it’s a mass death. One woman dying on the road? Routine.”
Distance Is a Death Sentence
In rural Jharkhand, especially in Latehar and Garhwa, 60% of the villages lie more than 10 km away from any functioning PHC. Add broken roads, no lights, and poor network coverage — and a 10-km journey becomes a 3-hour crisis.
In Banka, 65-year-old Mahesh Yadav had to carry his pregnant daughter on a cot with four others. The ambulance never came. “We were told to wait. We waited. And we lost her.”

She died in his lap 2 km before reaching the hospital. The baby was stillborn.
What Is a Woman’s Life Worth in Rural India?
Policy Promises vs. Ground Reality
The National Health Mission (NHM) allocates crores every year to improve rural maternal healthcare. In FY 2023–24, Bihar and Jharkhand received over ₹3,400 crore collectively.
But the real picture?
-
Only 48% of CHCs in Bihar have 24×7 delivery services
-
Less than 30% of PHCs in Jharkhand have full-time doctors
-
Maternal Death Review (MDR) mechanisms exist but are rarely conducted in actual field cases
Every scheme — Janani Suraksha Yojana (JSY), Janani Shishu Suraksha Karyakram (JSSK), Ayushman Bharat — fails in last-mile delivery.
Not because of lack of funds.
But due to corruption, apathy, vacancy, and distance.
Doctor Unavailable. Call tomorrow.
Our team visited the CHC in Sultanganj, Bihar, at 11:40 AM on a weekday. No doctor. No nurse in the delivery room. Just a ward boy playing games on his phone.
A woman in labor was lying on the hospital bench. Her husband was crying. A nurse showed up finally and said, “Ghabraiye nahi, sab theek ho jaayega” — but the delivery happened in the corridor.
We asked for the medical officer. We were told:
“He comes at 12:30. Maybe. Maybe not.” This story repeats every day, everywhere.
A System That Silences Grief
In Jharkhand’s Garhwa, when a mother died during childbirth in 2022, the family filed a complaint. But they were pressured to “settle” it quietly by offering compensation — ₹25,000.
No FIR. No disciplinary action. The ASHA worker was suspended temporarily.
A grieving mother-in-law said, “She died like an animal, without medicine, without a sheet, without a doctor. They said we should be grateful we got the body back.”
Conclusion — When the Womb Becomes a War Zone
What is left to say when mothers are dying not due to rare complications but because of predictable, preventable negligence? In India’s villages, childbirth is not a celebration — it’s a gamble with life.
While policies are launched on stage with fanfare, women die in the shadows of the system. Their stories don’t trend. Their pain doesn’t go viral. Their names are unknown. But if a nation must be judged by how it treats its most vulnerable, then India’s rural women are screaming the loudest into the void.
And no one is listening.